Gender and intersecting inequalities in access to health services
Timely access to good-quality, affordable healthcare (both preventive and curative) plays a critical role in maintaining good health. It is considered an important social determinant of health (WHO, 2019e). In the EU context, access to health services has been acknowledged as a right and recognised as a key principle of the European Pillar of Social Rights. In a survey carried out by EIGE, respondents ranked nine public services in order of the extent to which they enabled their participation in different everyday life activities[1]. The respondents, women and men alike, ranked health services as the most important type of public service and those that have the most transformative potential towards advancing gender equality in society. They create opportunities for people to be involved in education, employment and leisure (EIGE, 2020d).
Despite the EU standing out among industrialised regions for the health coverage of its population (OECD, 2019), universal access to health services is not yet achieved, and there are great variations in the level of access across the EU (Burns et al., 2019). Ethnic minority groups and migrant populations are seen to be over-represented among the population without, or with inadequate, health coverage (OECD, 2019). This section analyses which population groups are lagging behind in terms of access to health services and explores some of the reasons behind this.
Gender intersects with other social positions to hamper access to healthcare
Gender inequalities and gender norms intersect with socioeconomic, geographic and cultural factors and create structural barriers when accessing healthcare (WHO, 2019a). As highlighted in the domain of health chapter (Figure 22), several population groups, such as lone parents, older people, migrants and people with disabilities, and women in particular, stand out as highly vulnerable to unmet healthcare needs. Gender is an important determinant of healthcare access and uptake. Gender socialisation tends to deter men from seeking diagnosis and treatment, resulting in men being less likely than women to visit medical practitioners. A study in the United Kingdom found that men were 8 % less likely to consult a doctor than women, even when excluding consultations for reproductive reasons (Wang et al., 2013). The fact that women’s greater familiarity with the health and social services system is often attributed to the fact that they dedicate more of their time to childcare and long-term care.
Globally, people with disabilities have unequal access to healthcare services, and therefore have more unmet healthcare needs than the general population (WHO and World Bank, 2011). At the EU level, 7 % of women and 6 % of men with disabilities report unmet needs for medical services, but these figures are much higher in Estonia (29 % of women and 23 % of men), Romania (25 % of women and 23 % of men) and Greece (25 % of women and 22 % of men) (Figure 36). Gender gaps are modest in the majority of countries, with the exception of Estonia (6 p.p.). In Denmark, Sweden, Hungary, Bulgaria, the Netherlands and Luxembourg, men with disabilities are more prone than women to having their medical needs unmet.
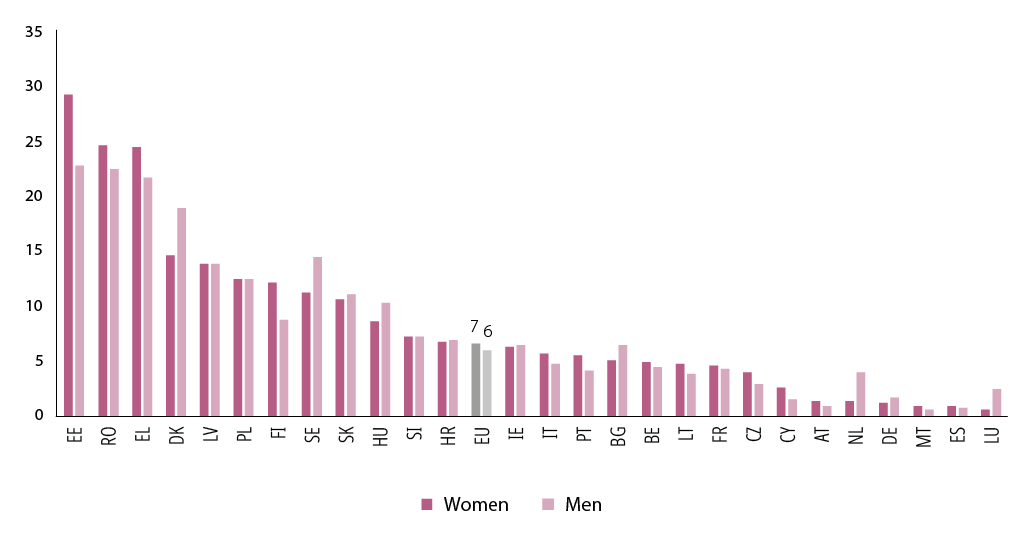
Figure 36. Unmet needs for medical services for women and men with disabilities, by EU Member State (%, 16+ years, 2019)
Source: Author’s calculation with microdata, EU-SILC, 2019 (IE, IT, 2018).
Older adults with disabilities and those living in rural areas experience difficulties in accessing appropriate transport to get to their medical healthcare providers (Gibson and O’Connor, 2010). Physical or structural barriers make it difficult for women with disabilities, especially when they live in rural areas, to access healthcare services, and as a result they may be dissuaded from attending screening for cervical or breast cancer (Ramjan et al., 2016). Furthermore, people with disabilities may have poor access to health promotion and disease prevention initiatives. This results in women with disabilities being less likely to receive screening for breast and cervical cancer than women without disabilities, and men with disabilities are less likely to be screened for prostate cancer (WHO and World Bank, 2011). The recently adopted 2021–2030 strategy on the rights of persons with disabilities includes access to healthcare[2]. The European Commission is also planning some guidance on access to healthcare based on inclusive, accessible, person-centred healthcare and free and informed consent, in line with the objectives of the UN Convention on the Rights of Persons with Disabilities.
Beyond medical services, access to long-term care services is critical to autonomous living and the well-being of people with disabilities and health limitations, especially in the context of the EU’s ageing population (EIGE, 2020f, 2021d). As shown by EIGE (2020f), barriers to accessing professional home-based care ae affect women disproportionately, as they are over-represented among the population most in need. In the EU, about 29 % of households reported unmet need for professional home care services in 2016 (EIGE, 2019d). Households were slightly more likely to report unmet needs (30 %) if a woman completed the survey than if a man did so (28 %). Women are more likely than men to report an unmet need for professional home care services in all but five Member States (LU, NL, AT, PT and SE) and the United Kingdom. The Member States with the highest unmet needs for professional home care services were Portugal (reported by 85 % of women and 86 % of men), Greece and Cyprus.
Nearly a quarter of women and men live in households that rely on informal care, which may either be insufficient or not be the most suitable / preferred arrangement for either the carer or the one cared for.
Access to palliative care or end-of-life care is also very uneven across the EU. Because palliative care revolves around pain relief and contributes to easing the physical and emotional suffering of patients and families, it is considered fundamental to human dignity (Council of Europe, 2018). The Council of Europe has highlighted the need to factor in rising needs for palliative care services as a corollary of ageing and an increase in the burden of disability. It raised particular concerns over ‘the lack of access to appropriate pain relief leading to situations in which patients suffer for months and even years and experience avoidable painful deaths’. Limited palliative care services have profound gendered impacts, with women bearing the brunt of lack of services not only as patients (women being more likely to suffer from health limitations, especially in older age groups, as shown in Figure 26) but also as informal carers whose own well-being and financial independence is put at risk by the burden of care (EIGE, 2019c, 2020e; Eurofound, 2020; Gott et al., 2020).
Reasons for unmet needs and underutilisation of medical services
This section will touch on three main sets of factors inhibiting access to medical services, namely the cost associated with them, experiences of discrimination and issues related to cultural sensitivity and a lack of gender sensitivity.
While unmet needs for medical services is a self-reported measure and, as such, could reflect certain biases, exploring reasons why individuals are not accessing the medical services they need can point to certain important determinants and inequalities and how they affect certain groups in particular.
Cost
According to EU-SILC data, about one quarter of individuals who reported unmet medical needs gave cost as a reason for being unable to access care (‘Could not afford to (too expensive)’). The other most common reasons for unmet medical care needs were ‘Wanted to wait and see if problem got better on its own’, lack of time (‘Could not take time because of work, care for children or for others’) and waiting times. In the case of dental care, the proportion of unmet needs due to financial reasons is far higher: half of the respondents gave this as an explanation. Women were a little more likely than men to mention cost as the main reason for not consulting, for either medical or dental care (Chaupain-Guillot and Guillot, 2015). Likewise, the cost of healthcare is a reason why women in financially unstable situations avoid care services, for example those who experience homelessness (Kneck et al., 2021).
As highlighted in Section 7.2., on the domain of health, women aged over 65 are slightly more likely than women overall to experience unmet needs for medical services[3]. The share of women and men aged 65+ experiencing unmet needs is highest in Estonia (22 % of women and 15 % of men), Romania and Greece (18 % of men and 13 % of women)[4]. Difficulties in accessing healthcare in old age are related to the fact that women are at higher risk of poverty or social exclusion than men when they reach old age (EIGE, 2020g), which reflects the accumulation of economic inequality over the life course. This is of particular importance since women are more likely than men to experience health limitations in old age (Ogg and Rašticová, 2020). Among people aged 65 and older, the leading reasons for unmet medical needs are affordability, especially among women, followed by being on a waiting list. Men are more likely than women to delay medical examination in the hope that the health issue will resolve itself (Figure 37).
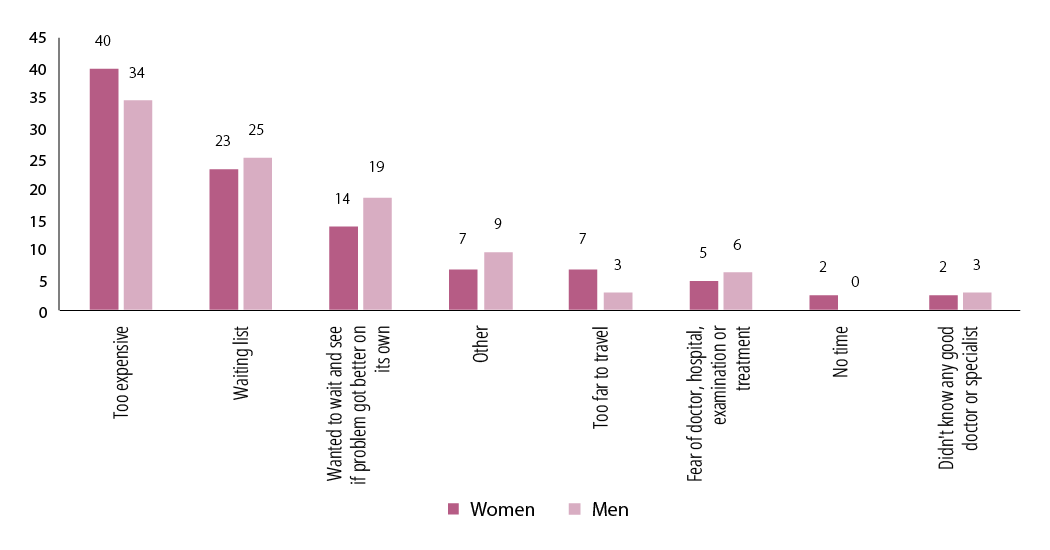
Figure 37. Reasons for unmet needs for medical examinations among women and men (%, 65+ years, EU, 2019)
Source: Authors’ calculations based on Eurostat, https://ec.europa.eu/eurostat/web/products-datasets/-/hlth_silc_14.
Cost of medical services as a barrier to access is more frequently mentioned by people aged 65 and over than in the adult population as a whole (40 % of women and 34 % of men aged 65 and over, compared with 33 % of women and 29 % of men of the total adult population).
This is not to say that other population groups are not experiencing difficulties in affording healthcare. Data shows that large segments of the EU population would find it difficult to pay for unexpected dental care (41 % of women and 35 % of men), mental health services (39 % of women and 33 % of men) and other hospital or medical specialist services (32 % of women and 29 % of men) (Figure 38).
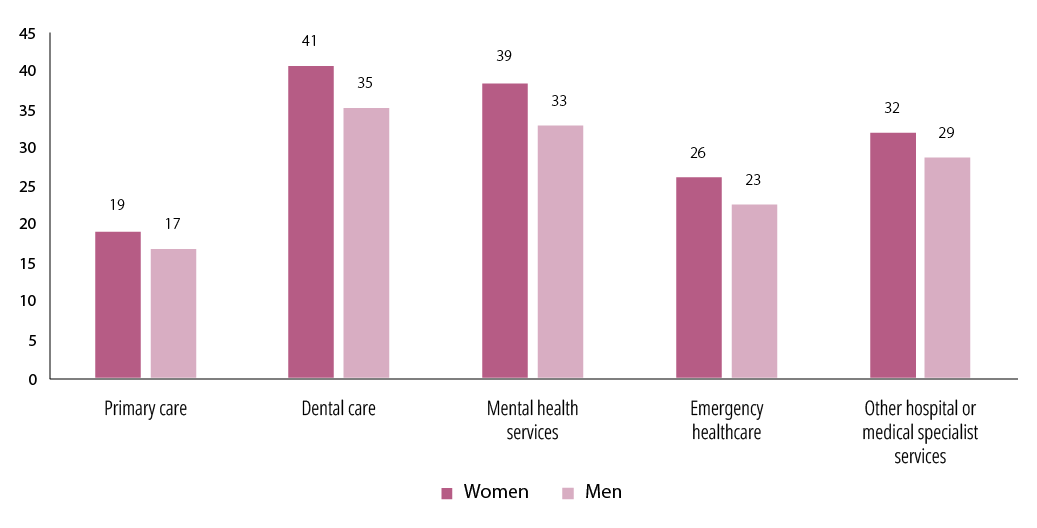
Figure 38. Difficulties in paying for unexpected medical expenses by sex and type of medical service (rather difficult or very difficult, %, 18+ years, EU, 2016)
NB: Respondents were asked, for each type of medical service, ‘How easy or difficult would it be for you to cover expenses for each of the following services, if you needed to use it tomorrow?’. Answers selected: ‘Rather difficult’ and ‘Very difficult’.
Source: EQLS, 2016.
The financial impact of health expenses, especially on a low-income population, can be captured by two indicators, namely ‘catastrophic health spending’, a situation in which households spend a high proportion of their resources on healthcare via out-of-pocket payments, and ‘impoverishing health spending’, in which a household either falls below the poverty line as a result of health expenses or is further impoverished by them (OECD, 2019). While ‘impoverishing health spending’ affects up to 6 % of households, catastrophic health spending is more common across the EU, affecting from around 1 % of households in Slovenia, Czechia and Ireland to 15 % in Lithuania (WHO, 2019b). Across the EU, households at the bottom of the income ladder, a group among which women and lone mothers are over-represented, were considerably more likely to be affected.
Discrimination and other systemic barriers
Accessing health services involves social interactions between patients and health workers in which societal power relations shape patients’ experiences (WHO Regional Office for Europe, 2016b). WHO’s 2019 global monitoring report on primary healthcare sheds light on how gender norms and power influence access to health services. The report found that gender norms and power relations influence women’s access to health services and timely diagnosis, while harmful notions of masculinity increase men’s risk-taking and reduce their willingness to use health services (WHO, 2019f).
Age, wealth, marital status, ethnicity, religion, caste, disability, education level, homelessness and migration status can lead to stigma and discrimination, which influence access to and use of health services (WHO, 2019a).
A survey by FRA found that 16 % of respondents felt discriminated against by healthcare or social services staff because of being LGBTI in the preceding 12 months[5]. Trans and intersex people were the most affected, with 34 % of respondents reporting feeling discriminated against in a health context, followed by lesbian women (16 %), bisexual women (14 %), gay men (11 %) and bisexual men (10 %). Members of the LGBTI community are still, at times, refused healthcare services or experience discrimination, and many feel unable to be open with healthcare professionals about their sexual and/or gender identity, or about being intersex. In the EU-28, 46 % of LGBTI respondents reported that none of their medical providers was aware of their LGBTI status. However, this figure varied greatly by country, from 28 % in Denmark to 82 % in Lithuania[6]. Discriminative behaviours experienced by LGBTQI individuals include stigma, denial or refusal of healthcare, and verbal or physical abuse. Knowledge and educational levels, beliefs and religion affect healthcare providers’ attitudes towards LGBTQI patients and can lead to homophobic behaviour (Ayhan et al., 2020). Heterosexism, transphobia and homophobia are barriers to healthcare service access; these phenomena are systemic factors, not just individual practices, and may cause LGBTQI people to avoid treatment altogether (Smalley, 2018).