Lone parents and people with disabilities are still without the health support they need
Across the EU, women and men report similar level of access to medical and dental examination in 2017: 97 % of women and men reported no unmets need for medical examination. Nevertheless, unmet healthcare needs were higher for certain population groups in the EU-28 in 2017 (Figure 31), especially lone mothers and fathers (6 % and 8 % respectively) and women and men with disabilities (8 % and 7 % respectively). At the Member State level, figures differed considerably. In Greece, Romania and Estonia, the share of women with disabilities lacking access to medical care was 30 %, 23 % and 22 % respectively. In contrast, in Member States such as Spain, Malta, Austria and Germany women with disabilities reported the same level of medical access as women without disabilities.
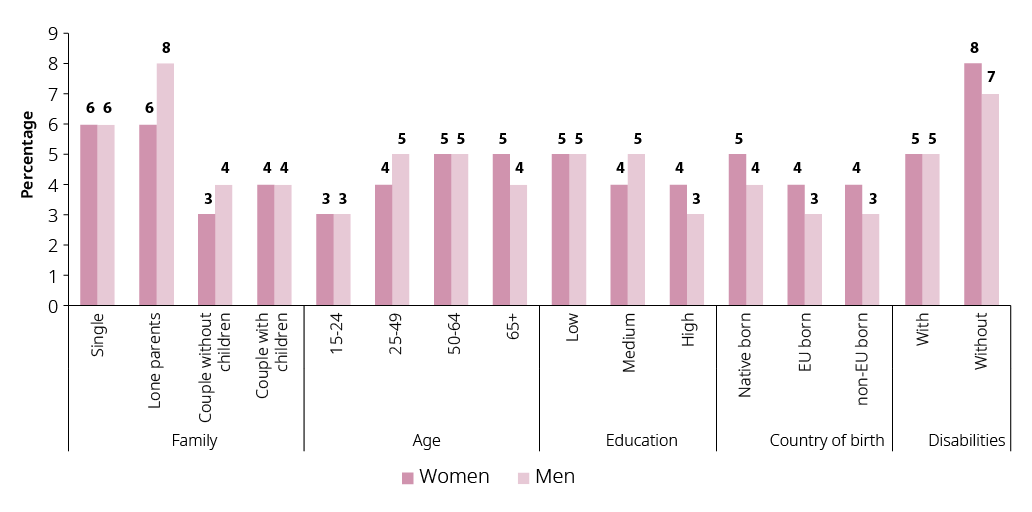
Figure 31: Women and men who report unmet medical needs by family type, age, level of education, country of birth and disability status (16+, %), EU, 2017
Note: EU-born and non-EU born are based on data from 23 of the 28 EU Member States: data is missing for Germany, Estonia, Latvia, Malta and Slovenia.
Compared to 2014, fewer women and men are reporting unmet needs for medical examination, particularly lone mothers. While 12 % of them reported this in 2014, only 6 % did so in 2017. Similarly, the share of women and men with disabilities reporting unmet medical examination needs shrank from 8 % for women and 7 % for women in 2014 to 13 % for both women and men in 2017.
The mortality rate for infections, blood and cardiovascular diseases and external causes was higher among migrants and refugees because of poor living conditions and lack of heathcare (WHO, 2018). In fact, migrants and refugees, especially those in an irregular situation, have unequal access to preventive healthcare across the EU, notably due to differences between Member States in access requirements for health services (WHO, 2018). Migrant and refugee women may face additional problems related to reproductive health (European Parliament, 2016). For example, undocumented pregnant women are more vulnerable to complications in pregnancy and childbirth throughout the EU (WHO, 2016).
Furthermore, as inequalities in health are often determined by education and socioeconomic status, people in the highest income quintile are more likely to report being in good health compared to people with the lowest income (OECD, 2017). Socioeconomic status and gender play a role in diseases and risk factors that contribute substantially to disability and lower quality of life. For example, people with a lower level of education are more likely to smoke, with evidence suggesting a more pronounced link among women.
Although wealthy women are the first to start smoking, they are also the first to stop. Disadvantaged groups, such as the long-term unemployed and homeless people, tend to smoke more in comparison with the more affluent. Research from Member States such as the Netherlands and Luxembourg suggests the trend of smoking is especially worrying among women with a low level of education (Hiscock, Bauld, Amos, Fidler, & Munafò, 2012; Nagelhout et al., 2012; WHO, 2016). Research in 17 European Member States also shows that people with a low level of qualifications are twice likely to die from excessive alcohol consumption compared to the most highly qualified (WHO, 2016).
Low educational levels and poverty often intersect with other aspects, such as ethnicity, to further exacerbate health inequities. Europe’s largest ethnic minority, the Roma, for example, face serious barriers accessing healthcare (European Public Health Alliance, 2018), with access to sexual and reproductive health services being particularly difficult for Roma women (Hoctor & Lamačková, 2017).
Although a minority group present across the EU, no systematic comparable data exists on the health situation of LGBTQI* people. Studies in different Member States, however, suggest that LGBTQI* people face significant health inequalities due to heteronormativity[1] in health systems, minority stress, victimisation and discrimination compounded by stigma (Zeeman et al., 2018). Evidence collected in OECD countries shows that there are higher rates of physical and mental health problems, particularly among transgender and intersex people (Valfort, 2017). For instance, LGBTI people were more likely to have considered or attempted suicide than those among the non-LGBTI population.
Evidence suggests that this gap has decreased more significantly among the US states that adopted same-sex marriage than those that did not (Valfort, 2017). Meanwhile, LGBTI employees in committed same-sex relationships who are not provided with the corporate-sponsored health insurance that employers give to workers in opposite sex marriages are at greater health risk from a lack of health insurance (Valfort, 2017). The social exclusion and discrimination faced by LGBT people in the labour market (FRA, 2014c) has also been closely linked to transgender people becoming become sex workers, consequently increasing their risk of and the prevalence of HIV (Valfort, 2017).