Rights, access and outcomes – sexual and reproductive health in focus
‘Good sexual and reproductive health is a state of complete physical, mental and social well-being in all matters relating to the reproductive system. It implies that people are able to have a satisfying and safe sex life, the capability to reproduce, and the freedom to decide if, when, and how often to do so’ (UNFPA, 2021).
The 1994 International Conference on Population and Development (ICPD) framed SRH as a basic human right. Building on landmark agreements of the ICPD in Cairo and the Fourth World Conference on Women in Beijing (1995), governments and advocates have worked to realise and expand international commitments on SRH. Since then, the protection and promotion of SRH without any discrimination, while tackling gender inequalities on this issue, have been on UN agendas and included in the SDGs.
Gender inequalities significantly impact SRH outcomes. They are shaped and structured in accordance with gender norms and unequal power relations in society, and may strip women and men of their ability to control their SRHR. However, biological sex determines the extent to which an individual can access SRH. Women, in particular, are subjected to sexual and reproductive control and limited in their bodily autonomy (UNFPA, 2021). Inequalities based on age, (dis)ability, race, ethnicity, migration status and sexual orientation, as well as gender, influence access to SRH. This section looks specifically at family planning and birth control, sexually transmitted infections (STIs) and STDs, and abortion and pregnancies. It also explores SRH developments during the COVID-19 pandemic. Gender-based violence is considered a contributing factor to poor SRH, and specific findings are included where relevant.
Gender-sensitive approaches to sexual and reproductive health are key to public health
Women and men have different SRH needs, and gender-specific approaches to SRHR highlight sex-specific diseases, for example breast or prostate cancer. Unique challenges in this area constrain the health of both women and men.
Women may experience a range of gynaecological conditions influencing their SRH. Issues relating to the female reproductive cycle – from menstruation to menopause – including painful periods and endometriosis, are particularly common. Other SRH problems faced by women and girls are uterine fibroids, interstitial cystitis, polycystic ovary syndrome, infertility of various causes, limited access to abortion, and the impacts of sexualised violence. Unplanned pregnancies, complications around pregnancy and childbirth, unsafe abortions, gender-based violence, STIs, STDs and reproductive cancers threaten the well-being not only of women, but also of men and families (Starrs et al., 2018).
Men’s reproductive health issues include male factor infertility, androgen deficiency, undescended testis, testis mass, scrotal disorders, phimosis, congenital chordee, Peyronie’s disease, premature ejaculation and sexual dysfunction, as well as concerns over contraception, HIV infection and STIs (Wessells, 2021).
Gender-biased reproductive health often overlooks men
Counselling, access to information and services, and birth control methods used to avoid unintended pregnancy enable people to make informed choices in their sex lives. Starrs et al. (2018) state that modern contraception was arguably the most revolutionary intervention in SRH in the 20th century, facilitating the delinking of sex and reproduction and enabling couples and individuals to choose the number and timing of their children.
On average, almost 95 % of family planning needs are met among women in the EU, but differences remain between Member States. In Slovenia, only 3 % of women and girls report having unmet needs for family planning, but in Spain this figure is more than double that (8 %) (Figure 39).

Figure 39. Women reporting unmet need for family planning, any method, by EU Member State (%, 15–49 years, 2017)
Note: Percentage of women of reproductive age (15 -49 years) who want to stop or delay childbearing but are not using a method of contraception.
Source: UN database, family planning indicators, https://www.un.org/development/desa/pd/data/family-planning-indicators, 2017.
Studies from Europe and worldwide show that family planning and birth control methods largely remain women’s responsibility, with men frequently kept out of the contraceptive decision-making process (de Irala et al., 2011; Dereuddre et al., 2017). Although contraceptive options include methods for men, and some require their participation, family planning programming has predominantly focused on women. Contraceptive options and methods follow a gender-binary approach in their design, since they concern male condoms and female hormonal contraception, for example the pill or injections. Female condoms have existed for decades, but are either less known or perceived as too expensive in comparison with the male version (Peters et al., 2010). Similarly, male hormonal contraception is still under development, with clinical trials previously being interrupted because of side effects such as dizziness, depression and changes in weight (Yuen et al., 2020).
In their literature review covering Europe, Canada and the United States, Gold et al. (2021) found that ambivalence towards pregnancy, miscommunication between sex partners and/or between patients and healthcare professionals increase women’s inconsistent contraceptive use. Research on men’s contraceptive behaviour is still limited, but findings from France suggest that miscommunication with partners also seems to contribute to unplanned pregnancies. Half of male survey respondents who had not used contraception, leading to an unplanned pregnancy, said they thought their female partners were using birth control (Kågesten et al., 2015).
Contraception availability and accessibility are not the only criteria for uptake. Reliable supply and low-cost interventions are other crucial factors for SRH outcomes. In Romania, Roma women have access to and know about contraceptives, for example the pill, injections and intrauterine devices, but they cannot necessarily afford them long term. Free SRH programmes are often discontinued or are not affordable because of transportation costs or corrupt health staff demanding bribes from Roma women (Kühlbrandt, 2019).
Overall, the UN estimates that 59 % of women in the EU can cover their contraception needs, with Finland outperforming all other Member States (Figure 40). However, data on contraceptive prevalence is lacking for men and for those defining their gender identity differently.
Male condoms and female hormonal contraception are the most prevalent birth control methods used by adolescents in the EU. On average, 65 % of 15-year-old girls and boys report using male condoms during their last intercourse, with the pill used by 28 % (WHO Regional Office for Europe, 2020a). A quarter of adolescents do not use either during intercourse, while more than a third in Croatia, Lithuania, Malta and Slovakia report not using any contraceptives (Inchley et al., 2020). Contraceptive access, availability, affordability and accountability vary greatly between Member States. According to the latest European Contraception Atlas (2020)[2], only seven Member States have comprehensive contraception policies (BE, DE, FR, LU, NL, PT and SE). Eastern European Member States (CZ, LT, HU, PL and SK) are the worst performing, although only in Poland has access to contraception been further restricted in the last 4 years. However, it should be noted that limited access to contraception is not associated with increased fertility rates: the 10 countries with the lowest access to contraception have lower fertility rates than the 10 countries with the highest contraception access.
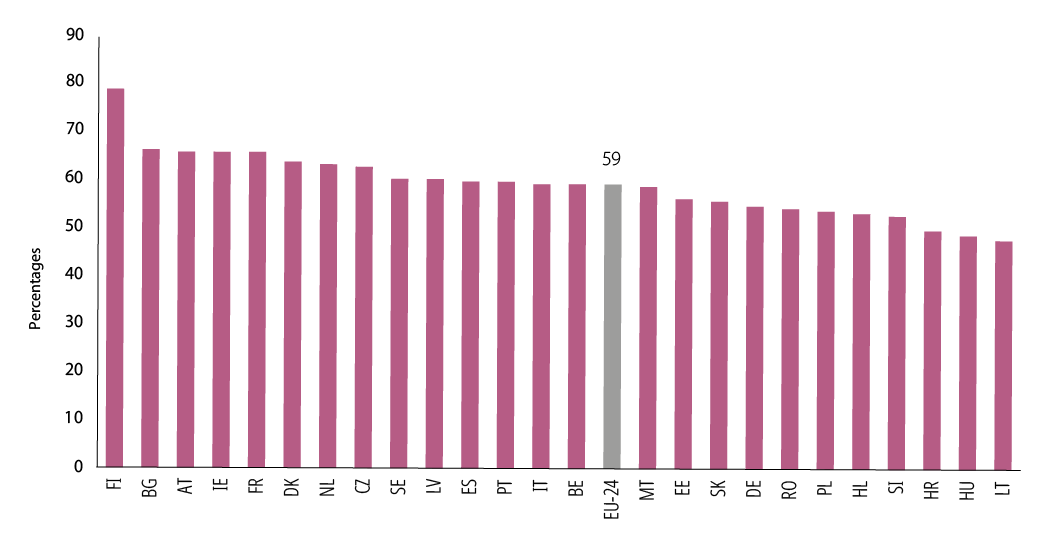
Figure 40. Estimated prevalence of contraceptive use of any method among women, by EU Member State (%, 15–49 years, 2020)
Note: Percentage of women of reproductive age (15-49 years) who are currently using any method of contraception
Citation: United Nations, Department of Economic and Social Affairs, Population Division (2021). Model-based Estimates and Projections of Family Planning Indicators 2021, custom data acquired via website. Source: UN database, 2020.
Women and men both vital to stop sexually transmitted illnesses
Not only do contraceptive methods help prevent pregnancies, but barrier methods such as condoms also make sex safer by limiting the spread of STDs and STIs. The most common STI in the EU is chlamydia, in many cases a symptomless infection in both women and men. Safer sex habits and testing are, therefore, essential tools to stop chlamydia from spreading. Infection rates are highest among women younger than 24 years (ECDC, 2020a), but social stigma can result in young women often avoiding chlamydia testing (Balfe et al., 2010). However, understanding men’s risk-taking behaviour can play an important role in preventing the spread of chlamydia. A study of young Swedish men tested for STDs revealed a variety of sexual risk behaviours and reasons why different subgroups did not use condoms. Migrant men reported more unprotected sex and more sexual partners overall, while men who have sex with men reported greater exposure to coercion to have unprotected sex (Helsing et al., 2021). Therefore, chlamydia prevention cannot solely rely on testing and safer sex practices. External factors, such as gender-based violence and gendered social stigma, also need to be taken into consideration in prevention policies.
According to WHO (2016c) and ECDC (2019) data, gonorrhoea is increasingly resistant to conventional antibiotics in Europe. Although this heightens the health risk for all people, gender implications need attention. While infertility is a serious consequence of an untreated gonorrhoeal infection for women and men, it is also associated with adverse pregnancy outcomes. Mother-to-child transmission of gonorrhoea can cause blindness in the newborn (WHO, 2016b). Since gonorrhoea is mostly asymptomatic, especially in women, women partners of those diagnosed should be screened. Prevention efforts should also include the supply of male and female condoms (Ndowa et al., 2012).
Abortion, pregnancy and maternal care disparities across the European Union
Estimates suggest that almost half (48 %) of pregnancies worldwide are unplanned (Bearak et al., 2020). This shows that abortion services and care are essential components of public health, to ensure high-quality SRH for women and girls (WHO, 2012). The physical and mental health of women and girls who have an abortion requires more than just that the procedure is medically safe. Abortion can be considered safe only when it is performed without the risk of criminal or legal sanction, stigmatisation, stress or isolation (Starrs et al., 2018). Laws and policies on accessing abortion services, with reproductive health consequences for those using them, vary greatly across Europe. Although barriers to legal abortions differ across the EU, all Member States except one allow it under certain conditions. In Malta, all abortions are banned (IPPF, 2019).
Eleven Member States – Belgium, Germany, Ireland, Spain, Italy, Latvia, Luxembourg, Hungary, the Netherlands, Portugal and Slovakia – have a mandatory waiting period. Belgium, Germany, Italy, Lithuania, Hungary, the Netherlands and Slovakia mandate pre-abortion counselling. The only countries not requiring third-party consent, for example parental consent, for abortion in underaged children, are Belgium, Ireland, the Netherlands, Portugal and Finland (IPPF, 2019). Legal provisions can change in both directions: more liberal abortion policies were recently adopted in Ireland (UNFPA, 2021), while Poland tightened its already restrictive abortion legislation in 2020. Overall, eastern European Member States have the most unwanted pregnancies and 66% of unintended pregnancies end in abortion here (Bearak et al., 2020). They also rank low on the Contraception Atlas (2020), suggesting inadequate SRHR policies. According to the most recent WHO data available (2015–17)[3], the fewest abortions in the EU are in Member States with the most restrictive abortion laws – Ireland[4], Malta and Poland.
Lastly, many abortions are carried out unregistered, either by medical staff or outside the healthcare system altogether, which can explain that in the UN European region, between 2010 and 2014, 11 % of all abortions were deemed unsafe (Ganatra et al., 2017). The same study also found that countries with highly restrictive abortion laws and policies had a higher share of unsafe abortions than countries with less restrictive laws.
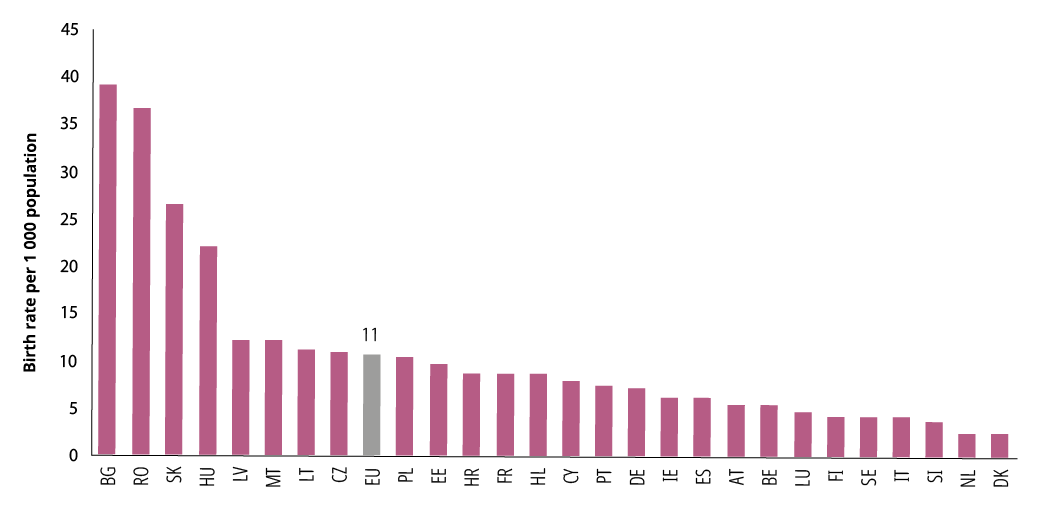
Figure 41. Adolescent birth rate by EU Member State (per 1 000 population, 15–19 years, 2018)
Source: SDG 3.7.2., UN, https://unstats.un.org/sdgs/unsdg, 2018.
Sexuality education is essential to prevent unplanned pregnancies in adolescence. Young people are in need of comprehensive sexuality education to understand and enact their rights to health, well-being and dignity. Access to rights-based sexuality and relationship education varies between Member States (EIGE, 2020a). The German Federal Centre for Health Education (BZgA)[5] developed sexuality education standards for Europe in 2010 as a framework for policymakers, education and health authorities, and specialists (WHO Regional Office for Europe and BZgA, 2010). An assessment carried out in 2018 (BZgA and IPPF EN, 2018) found that the implementation of sexuality education differed widely between and within EU countries. While sexuality education is mandatory in most Member States (except Bulgaria, Italy, Cyprus, Lithuania, Poland and Romania), exemptions can be granted based on faith and moral grounds (EIGE, 2020a). Inadequate sexuality education, along with other factors, such as lack of access to contraceptives, can contribute to higher birth rates among adolescents. In the EU, birth rates in this group are highest in the eastern European Member States, with rates in Bulgaria, Hungary, Romania and Slovakia more than double the EU average (Figure 41). In these countries, sexuality education is optional, with students also start learning about sexual health issues later in their school life in comparison to their peers in other Member States. (Picken, 2020).
Maternal care inequalities persist, especially for migrants
Although maternal and child mortality has been steadily decreasing in the EU, pregnancy still carries health risks (WHO, 2017). Some health conditions occur only during or after pregnancy and require assessment from a gender-informed perspective. Researchers and practitioners alike have long overlooked several pre- and postnatal health conditions, with care in these areas requiring improvement. For example, hyperemesis gravidarum, or chronic morning sickness, affects an estimated 2–4 % of pregnancies and is potentially deadly (McCarthy et al., 2014). Yet it is often unrecognised by healthcare professionals and classified as something imagined or exaggerated by women suffering it (Jansen et al., 2020). Likewise, violence in childbirth, known as obstetric violence, poses a risk to maternal health in the EU[6].
UNICEF data shows that the maternal mortality ratio (per 100 000 live births) in the 27 Member States in 2017 ranged from 2 in Italy and Poland to 19 in Latvia and Romania. Maternal mortality and care inequalities are higher among marginalised and vulnerable communities such as migrants, refugees, asylum seekers, women with disabilities, prisoners and victims of trafficking. Access to maternal healthcare services and midwifery in the EU is affected by the interplay between health systems, laws, policies, socioeconomic factors and attitudes of healthcare professionals and users.